UPDATE: I forgot one argument of which readers reminded me: the “slippery slope argument.” To wit:
5. Assisted suicide laws could lead to a “slippery slope” condition whereby shady doctors allow people to be medically euthanized for curable conditions, or even to allow relatives to kill their grandmothers. Yes, this is a danger, though one that can be ameliorated with sufficient stringent vetting laws. The “kill your grandmother” argument can be prevented completely, and certifying certain doctors and shrinks for their objectivity in vetting would be another good step. But when weighed against the suffering eliminated by assisted dying laws, I think the slippery-slope argument, while surely worth considering, is outweighed.
________________________
Assisted suicide for people who have severe and incurable mental illness has always seemed a no-brainer to me, but I’m surprised at the number of people who push back when I bring this up. But, if the procedure is implemented properly, the objections to it don’t seem tenable, and in the end seem to resemble arguments against abortion. That is, the pusher-backers say that people in tough spots shouldn’t have control over their bodies, that the procedure might spread if it’s allowed, and, underneath the objections of many, we find religious feelings—in this case feelings like “God will take you when He’s ready, not when you’re ready.”
Yet it seems to me undeniable that some cases of mental illness, like the main one documented in the Free Press article below, are so severe that they resemble terminal illnesses—illnesses for which enlightened people would favor assisted suicide (I might use the term “euthanasia”) in this post. If you’re terminally depressed, in horrible mental pain all the time, constantly thinking about suicide, and have tried every possible remedy without any success, then why aren’t you in a position similar to that of a cancer patient who, having tried all remedies, now faces a finite term of horrible pain ending certain death? (I presume you’re aware that even in states not permitting assisted suicide, doctors often mercifully end the lives of such patients by giving them an overdose of morphine.)
The difference with mental illness is that death is not certain and the pain will last a lifetime. Sure, maybe researchers will come up with a cure for an intractable mental illness, but that also holds for terminal physical illnesses. People with bad prognoses often hope that a cure will be discovered before they die.
Now for the state to effect euthanasia, there must of course be restrictions. Beyond that, anybody has, in my view, the right to kill themselves by other means, like hanging, shooting, or jumping in front of a train. That kind of suicide is illegal, though I think the illegality is nuts. But for the government to help you die, it’s not proper to provide anybody with the means of euthanasia. There are many reasons, but I won’t enumerate them.
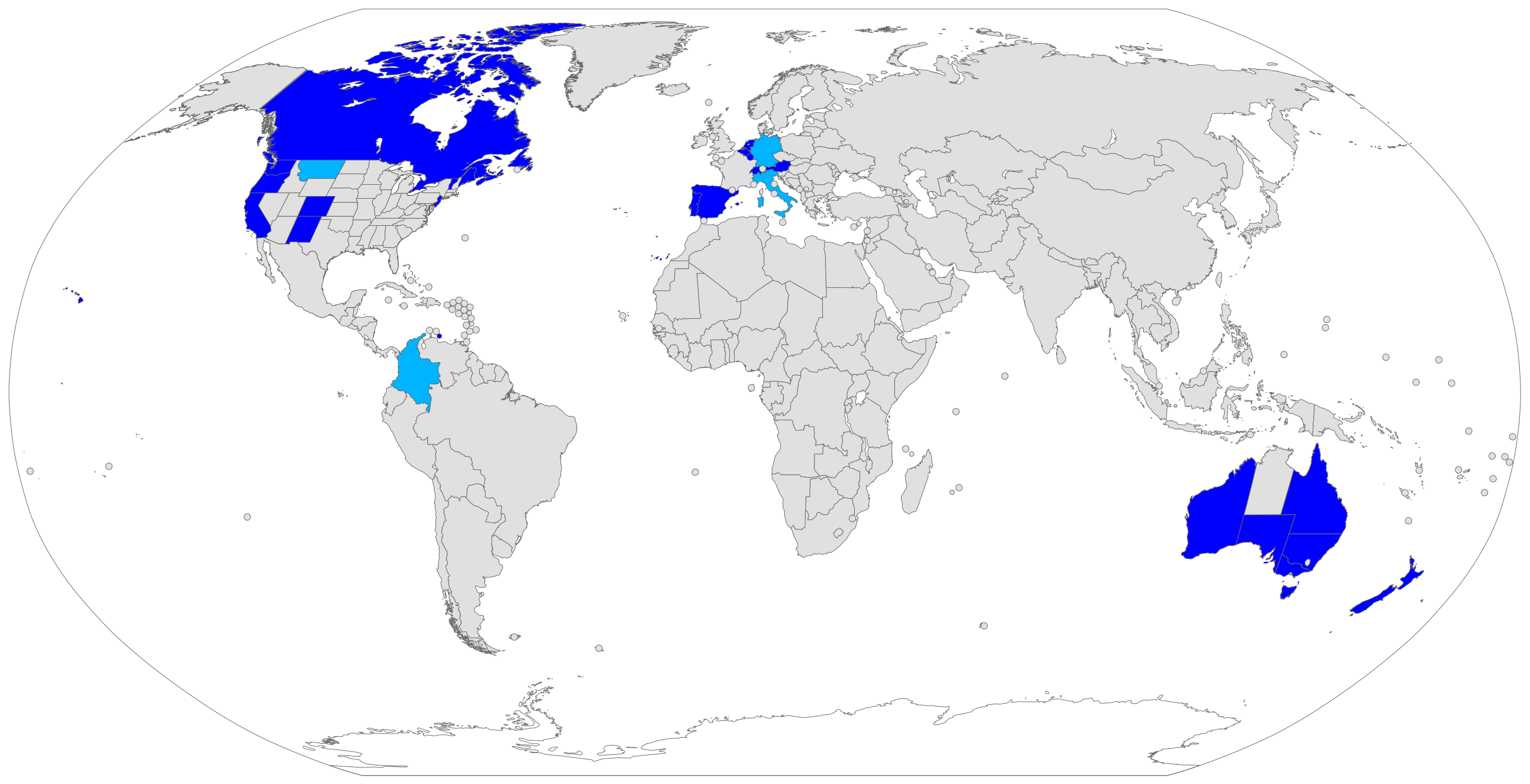
Naturally, in places where euthanasia is officially legal (see the map below), there are such restrictions for the physically ill:
Physician-assisted suicide is legal in some countries, under certain circumstances, including Austria, Belgium, Canada, Germany, Luxembourg, the Netherlands, New Zealand, Portugal, Spain, Switzerland, parts of the United States and all six states of Australia. The constitutional courts of Colombia, Germany and Italy legalized assisted suicide, but their governments have not legislated or regulated the practice yet.
In most of those states or countries, to qualify for legal assistance, individuals who seek a physician-assisted suicide must meet certain criteria, including: they are of sound mind, voluntarily and repeatedly expressing their wish to die, and taking the specified, lethal dose by their own hand. The laws vary in scope from place to place. In the United States, PAS [physician-assisted suicide] is limited to those who have a prognosis of six months or less to live. In other countries such as Germany, Canada, Switzerland, Spain, Italy, Austria, Belgium and the Netherlands, a terminal diagnosis is not a requirement and voluntary euthanasia is additionally allowed.
Below is a map of where assisted suicide is legal throughout the world, and there aren’t many places. The states in the U.S. where it’s legal include Maine, Hawaii, Washington D.C., Washington State, Colorado, New Mexico, New Jersey, Vermont, and Oregon. But in no state is assisted suicide permitted for those with mental illness. For physical illnesses or other conditions that are likely to kill you in a few months, here are the general criteria in the U.S.:
- an adult as defined by the state
- a resident of the state where the law is in effect
- capable of using the prescribed medications without assistance
- able to make your own healthcare decisions and communicate them
- living with a terminal illness that is expected to cause death within 6 months as verified by qualified healthcare professionals
Places where assisted dying is legal (see the key for variations):

Places that permit euthanasia for those with mental illnesses include only the Netherlands, Belgium, Luxembourg, Switzerland, and—perhaps after 2027—Canada. I haven’t looked up the criteria for state assistance for euthanasia for the mentally ill in all four countries, but here are the criteria for the Netherlands given in the Free Press article below by writer Rupa Subramanya.
Dutch law requires those seeking assisted suicide to show they are in great pain, have no alternative, and are acting of their own volition. They also must get sign-off from at least two doctors, including a psychiatrist. The process can take a few years, culminating with a doctor giving the patient a fatal medication or, if done by oneself, a cup filled with poison to drink. When it’s over, a government panel reviews the case to ensure everything was above board.
Click below to read the article. The woman pictured, Zoraya ter Beek, suffered her whole short life from depression, autism, and borderline personality disorder, and said she was in constant pain. Nothing helped, and eventually the doctors and shrinks said there was nothing more that they could do for her. Tired of living, she applied for and qualified for assisted suicide. She is still alive but scheduled to die in May. (That isn’t final, of course, for I’ve read of such patients who change their minds at the last minute, willing to go on but heartened by the fact that at any time they could choose to die.) Her boyfriend loves her, but agrees with her decision.

Here are some of the objections to assisted suicide for mental illness, and my responses (all text is mine).
1.) The patient could get better but, by taking their life, are depriving themselves of a livable and perhaps enjoyable future. Yes, but that’s true of even physical illnesses. Besides, the prognosis must be confirmed by several doctors and examined post facto by the state. And I would ask those who make this argument, “Who are you to tell someone that they must go on living when they’re in intractable pain?” For those of us who have been severely depressed, it’s hard to convey to others that this kind of severe and prolonged mental pain is fully capable of making you wish to die.
2.) It’s up to God to determine when you die, not you. As an atheist, or even as a rationalist, I find this argument bogus. Here it’s similar to the religious argument against abortion, assisted suicide for physical illnesses, or, as Peter Singer discusses, euthanasia for newborn babies who have a condition that will cause them to suffer and, ultimately, kill them with certainty in a short time. Besides, are you going to base medical decisions on assuming that there’s a god for which we have no good empirical evidence? Isn’t medical treatment supposed to be based on empirical criteria? Do you tell a dying atheist that you can’t increase the morphine drip because God doesn’t want that?
Here’s a quote from the article:
All this pointed to a “dystopian view of the future,” said Theo Boer, the healthcare ethics professor.
“Whether or not you’re religious, killing yourself, taking your own life, saying that I’m done with life before life is done with me, I think that reflects a poverty of spirit,” Boer told me.
. . . . Theo Boer, the bioethicist, acknowledged that none of the suicides in the Bible is condemned, but he added that they are not lionized or commemorated either.
“Suicide in the Bible belongs in the realm of the tragic, and the tragic should not be condemned—nor should it be regulated or celebrated,” he said.
This palaver, including the phrases “Life is done with me” and “poverty of spirit” seems to reflect religious belief, but it’s already clear from opposition to euthanasia in many places (especially the U.S.) that we shouldn’t cut short what is up to God to determine. But if God is omnipotent, wouldn’t He be behind a mentally ill person’s decision to have assisted euthanasia?
3.) It’s contagious. There are several statistics given in the article about assisted dying increasing over time. Most are for physical conditions, with only one for mental illness (my bolding)
In 2001, the Netherlands became the first country in the world to make euthanasia legal. Since then, the number of people who increasingly choose to die is startling.
In 2022, the most recent year for which there is data, Dutch officials recorded 8,720 cases of euthanasia, a 13.7 percent increase from 2021, when there were 7,666 cases. To put this in perspective, there were a total of 170,100 deaths in the Netherlands in 2022—meaning euthanasia cases comprised more than 5 percent.
“This upward trend, in both the absolute and relative numbers, has been visible for a number of years,” the country’s Regional Euthanasia Review Committee’s 2022 Annual Report states. What’s more, the number of euthanized people between the ages of 18 and 40 jumped from 77 in 2021 to 86 in 2022. And the number of people with psychiatric disorders who choose euthanasia is rising: In 2011, there were just 13 cases; in 2013, there were 42; and by 2021, there were 115.
This trend is not limited to the Netherlands. From 2018 to 2021, countries where euthanasia or assisted suicide is most popular saw sizable increases in the number of people signing up to die: In the United States, where ten states and the District of Columbia have physician-assisted suicide, there was a 53 percent jump; in Canada, 125 percent.
But why wouldn’t you expect the numbers to rise as people become aware that they have this alternative? It’s not written about very often, so you have to see articles like this to find out about it. But even so, this is a question of ethics, not of statistics. If the regulations are sufficiently rational and stringent that they prohibit spur-of-the-moment suicides or mental conditions for which every possible cure hasn’t been tried, why should we care about the increase? And wouldn’t you want the ability to die a peaceful and painless death if you had a condition that could be terminated in a peaceful way, at a time and place of your choosing, and when you are surrounded by loved ones? (This is, as I’ve learned, the way it usually occurs.)
4.) It hurts those who are left behind. I’ve heard this argument used often against those who discuss self-inflicted suicide. “If you kill yourself, think of all the people who will miss you and be in pain.” But this seems eminently selfish to me. Everybody who dies before their friends, relatives, and loved ones (and that means all of us) faces that as a certainty. If someone’s in intractable physical pain and dying of cancer, would you tell them to hang on for your sake? Of course not! The same holds for incurable mental illnesses. It’s selfish and boorish to ask someone to stay alive for the sake of your—or other people’s—feelings.
For #5, see the update at top.
For some people, suicide is simply a no-go zone, which is why suicide hotlines exist to talk those who wish to die out of that wish. But that’s different, for someone who calls a hotline has a good chance that they’re simply emitting a cry for help, and want to be talked out of it. (However, some do kill themselves.) That’s why I think those hotlines are great things. But assisted dying with stringent criteria needed to qualify, and the use of drugs that assure a painless death, are not equivalent to a suicide hotline.
I’m sure that ethical philosophers have discussed this issue before, and feel free to cite articles below if you know of them (I don’t). These are of course tentative ideas that I’ve thought about for a long time (note: I’m NOT a candidate!), and were given shape by the article above, but I’m willing to listen to other points of view. If you have them, or if you agree with what I’ve said, weigh in below. But do read the Free Press piece.
I agree that suicide should be legal. But I’m not sure I agree that jumping in front of a train is an ethically defensible way to do it.
One of my relatives is a train driver and suicides are an occupational risk. They take an enormous toll on the mental health of drivers. Nightmares, crippling guilt, PTSD, the whole awful nine yards. Some people have to stop driving trains entirely afterwards.
I don’t think it’s fair to inflict that much suffering on a stranger who’s just doing their job, even if it is to relieve your own suffering.
There are many other ways, and those other ways should be encouraged.
Yes, you make a good point, and I’d prefer a different way myself, but you can’t tell people who want to jump in front of a train that they can’t do it because it inflicts mental trauma on the engineer. So does shooting yourself in the head with a shotgun, as Hemingway did. If someone survives this, and you think they should be prosecuted for what is, after all, still an illegal act, be my guest.
Curious anecdotal information: some people attempt suicide with a gunshot to the temple but succeed only in severing the optic nerve thus blinding themselves. You’d think their urge for suicide would be increased but apparently not.
Is suicide (or attempted suicide) by your own hand illegal in any jurisdiction in what are loosely called Western countries? I’m surprised to read of suicide by the traditional means being described as illegal. It’s relevant to a comment I might make later. Canada repealed its law against attempting one’s own suicide in 1972.
(Google turns up only a few (~20) primitive and Muslim countries that make it illegal.)
I also do not see the difference between pain from mental illness and pain from a physical illness. I think this distinction is based on the dualist notion of free will. I am disheartened by governments that wring their hands over assisted suicide for those with mental illness but cheerily permit it for those with diseases like Parkinson’s or ALS (illnesses that also affect the brain and nervous system). I thought it wrong that Canada delayed their decision though I understand they were honouring the need to discuss it.
To me, the difference is that certain mental illnesses make the person unable or incompetent to take life-altering decisions, so the end-of-life decision will be taken by someone else – often a relative whose own life will be easier if the person with mental illness is no longer alive.
That’s not how the legislation works for mental or physical end of life decisions when it comes to medical assisted dying. You may be thinking of other situations but when you say you want MAID specifically if does not work that way.
Excerpt from
Science, Politics, and Gnosticism
Eric Voegelin
1968, 1997
Regenery Press, Chicago;
Washington D.C.
Bold added
[begin excerpt]
1) It must first be pointed out that the gnostic is dissatisfied with his situation. […]
2) Not quite so understandable is the second aspect of the gnostic attitude: the belief that the drawbacks of the situation can be attributed to the fact that the world is intrinsically poorly organized.
[…]
gnostics are not inclined to discover that human beings in general and they themselves in particular are inadequate. If in a given situation something is not as it should be, then the fault is to be found in the wickedness of the world.
3) The third characteristic is the belief that salvation from the evil of the world is possible.
[.skipping 4th point..]
5) […] belief that a change in the order of being lies in the realm of human action, that this salvational act is possible through man’s own effort.
6) If it is possible, however, so to work a structural change in the given order of being that we can be satisfied with it as a perfect one, then it becomes the task of the gnostic to seek out the prescription for such a change.
[end excerpt]
I’m not sure what to make of that but the intolerable mental pain that has no means of measurement – or I missed it – strikes me as a truth claim – a gnostic claim – accepted on faith. That can happen, like ringing ears – nobody can measure it but it is obvious. But nobody would schedule suicide for it (that I know of). Here, the change in the world was determined by the gnostic removing themselves from it.
Hard topic.
I think the majority of people regard MAID for the terminally ill as, at the least, a defensible position. I was a Canadian GP for 30 years, working in a rural area and running a small hospital. I did a lot of palliative care, and I know it is far from perfect, so I would have agreed to perform MAID for the terminally ill if I had still been at work when it came in.
But we are witnessing it being expanded to the mentally ill, the socially dependent, and even disabled children have been suggested in Québec as candidates. This is not something most of us are comfortable with. And it gets worse when the government begins to see this as an economically desirable tool for curtailing public expenditure. 6% of deaths in Quebec are now medically assisted, and across the country, there was a 30% rise in 2022 from the previous year. No doubt careful calculations of cost-savings are being performed in ministries that are responsible for spending on caring for needy citizens, and bureaucrats are licking their lips at the thought of how this would assist their budgets. The latest proposal is for ‘targeted organ donation’ which would allow someone choosing MAID to say in advance to whom their organs should go. How much of a free choice is it when your family member who needs a kidney starts to talk to you about “wouldn’t it be great if…”?
The slippery slope is no longer a theoretical risk: it is here and we have started the long slide downhill. And the government has an excuse—the Supreme Court of Canada has the ability under our Charter of Rights and Freedoms to dictate law to parliament, and that is what has happened. If the terminally ill have this right, it cannot be legally denied to other citizens, and so parliament has to come up with laws permitting it. When the Charter was written into our constitution in 1982, there was much debate about how this would change our legal and constitutional landscape, but this particular wrinkle was not predicted. Judicial oversight can go too far, and the ultimate authority should lie in an elected parliament answerable to the electorate and no one else. For some strange reason I am more comfortable with every suicidal adult having access to painless and guaranteed success than I am with a government offering to end things for citizens that are getting expensive to look after. Doctors ought not to be in the business of polishing people off, as it encourages bad habits (if you get my drift). Once you have your chit from the doc saying you are in your right mind, you present it to a pharmacist and get a pill and some instruction. Squeamish pharmacists may exclude themselves, or simply give a printed handout if they don’t want to describe the details, which would be something like “Go home. Swallow this pill. By the way, have you settled your bill here before you leave?”
As someone with an incurable cancer, I want my doctors to help me live as long and as well as possible. Only I should be able to say if I have had enough. Teaching our young physicians that death is always an option for difficult cases will, inevitably, corrode our doctors’ sense of what their duty to their patients should be. It places an unfair onus on the sick, the poor and the disabled to “do the right thing for society” rather than to make a free choice if they ever get to that stage. How much pressure might be applied to young physicians to go beyond the terminally ill and include these less clear-cut cases? It isn’t unimaginable that professional bodies would sanction physicians who were choosy or squeamish in this regard for discriminating against a class of applicants, just as we are no longer allowed to follow our conscience when it comes to declining to treat gender dysphoria without being punished. This is getting beyond a horror story: it’s a horror show and I want no part of it.
Christopher that is already true in Ontario. The licensing regulator says that for patients who qualify under whatever the federal criminal code’s murder exemption is this year, doctors must either do euthanasia on request or make a meaningful referral. This would mean that if the shadowy little band of current euthanasia doctors exits the business and no referrals are possible, the GP would have to look up the information about the drugs, helpfully published on the regulator’s website, and do the deed herself, like it or lump it.
The difficulty with compelling doctors to kill physically healthy people with mental illnesses on demand is that it could deter doctors from taking up the euthanasia craft, creating yet another reason to avoid primary care and having this sort of unpleasant obligation dropped in one’s lap because no one else will do it. Critics of the medical profession don’t trouble themselves with doctors’ moral distress—“Just give me what I want and keep your religion to yourself, Doctor”— I get that. But no one has to become a doctor. Telling high school students that they will end up being forced to kill healthy people and sterilize healthy children or lose their licences is not good marketing for the profession.
This is a difficult one for me. My wife is disabled, and she has let me know that, should she ever get a terminal diagnosis for cancer or the like (and she has a family history), she will move somewhere that euthanasia is legal.
Personally, I have always been against legalizing euthanasia, believing that legalizing assisted suicide is a slippery slope. These days, I don’t believe there are slippery slopes; I believe people are taking first steps in journeys they mean to complete. We have seen in Canada cases where people seeking medical aid (for instance, in getting a new wheelchair) had euthanasia suggested to them. Now doctors in both Belgium and Britain are arguing that simply being old is enough of a reason for assisted suicide.
The head of Belgium’s Christian Mutual Insurance said, “We have to remove the stigma between life and death.” I am sorry, but when you do that, it becomes possible to convince people that it is alright to kill people without illness in the name of cost, the environment, religion, or whatever the flavor of the moment is. We have seen that the line between mercy killing and murder is very fine. How often have we heard it said that people with certain political views were “insane”? If the “stigma between life and death” is removed, then governments can (and will) kill their opponents in the name of the greater good. Germany’s Aktion T4 really showed us all we need to know.
I suspect your wife wouldn’t take the “slippery slope” arguement that seriously given her condition (and my best wishes for her). It’s better to have the option with good, strict regulations than to not have the option at all. Or do you disagree? Do you think that NOBODY should be allowed to have assisted suicide because it’s all a “slippery slope”?
No, I can’t say never.
Food for thought. Removing the stigma between life and death is an important discussion, but among those cases you describe are some that go well over the line of ethics.
The question to ask is not whether assisting-dying in the case of mental illness is moral/not; but whether setting a legal precedent primes the stage for a diminished value for life. The data appears to back up my unease.
I am opposed to legalizing assisted ‘dying’ – in general. There are (of course) exceptions that are already legal.
Would like to write more, but am off trying to save a herd of precious African elephants (30-40) about to be eliminated (perhaps lethally) for simply being elephants. The story is more complex of course, but the point is that hardly any animal, except humans, and, mostly those humans in the “developed world” – obsess so intensely about life/death.
Is it a luxury to choose death? Maybe so. I don’t know.
I do know this: life is f-ing precious, all of it. Everyday, I see creatures around be struggling to live. Doing crazy shit, just so they can live another day.
And yes, some of us do suffer. Maybe many of us; that too is part of life. It’s called the human estate.
Live.
Rosemary, your observations about suffering on Earth are spot on. I agree, but I would not be satisfied with merely describing the state of affairs in this world of pain and pleasure. If ethics aims to reduce or even eliminate suffering, both human and animal, then suicide should be an option. After all, death is the blessed relief of all of our suffering.
Disclosure: In my 69 years on this planet, I’ve had five friends who have taken their lives. Three overdosed on pills; one went into his garage, closed the door, started his car, and inhaled the CO; one kissed the third rail of a Chicago El train railroad. Each was in immense pain, both physical and mental, for years before they ended it all. I wonder if assisted suicide/euthanasia would have made their deaths easier and less traumatic, not only to them but to their relatives and friends.
Unnecessary suffering is NOT a normal part of life. That’s why we invented central heating, refrigerators, trains, etc…
Allowing unbearable suffering to continue when it can be easily stopped is the immoral course of action. Strong guidelines are required, and even in my home country of Canada these regulations are fiercely debated.
Indeed. I would expand upon your point by saying that the arc of human ethical development has defined more and more things as “unnecessary suffering” that were considered “necessary suffering” in the past. Witness the advances in orthopedic surgery, which has eliminated many causes of joint pain. Psychiatry has also lessened some of the pain of mental illness, though I admit that there is much more that we need to do along this line. In general, any technology that makes it easier to accomplish our daily tasks reduces suffering.
Stephen, thank you for a thoughtful response. I remain unconvinced that legalizing suicide for humans with psychological issues (assisted dying in the case of emotional distress) will lead to a “better world” for all.
My niece took her life in 2022. I don’t judge her for her decision, never will, and will continue to grieve her loss; should her decision (at 19+) been legal and sanctioned by the state. I say vehemently – No. Suicide should remain an anomaly to *life*.
Yes, death is a relief from suffering, but the legalization of death in the form of assisted dying (particularly in the case of emotional distress) normalizes a way out.
It’s not a giant intellectual leap to “see” that the end-game of normalizing mental illness via legal avenues (currently sweeping the west – WEIT writes about it implicitly and explicitly), can and does lead to normalizing suicide; leading to more suicides; and -clearly- there are unforeseen consequences to legalizing suicide (see below) besides the alleviation of suffering.
The west appears to be obsessed with erasing all forms of pain, suffering, discipline, and long-term thinking/solutions from its cultural zeitgeist.
The author of the FP piece cited by WEIT (Rupa Subramanya) discussed her findings with Megyn Kelly, (below) her research suggests that in every region/state/country where assisted dying is legal, suicide (outside the purview of *assisted suicide*) has also risen. A form of ‘suicide contagion’.
“Disturbing Rise of Young People Dying By Suicide… Including Assisted Suicide, with Rupa Subramanya”
https://youtu.be/yYiIxCspsfM?si=XOz-YfWe4iz6-SaB
Also, from the article: https://www.thefp.com/p/im-28-and-im-scheduled-to-die
“Theo Boer, a healthcare ethics professor at Protestant Theological University in Groningen, served for a decade on a euthanasia review board in the Netherlands. “I entered the review committee in 2005, and I was there until 2014,” Boer told me. “In those years, I saw the Dutch euthanasia practice evolve from death being a last resort to death being a default option.” He ultimately resigned.
Boer had in mind people like Zoraya ter Beek—who, critics argue, have been tacitly encouraged to kill themselves by laws that destigmatize suicide, a social media culture that glamorizes it, and radical right-to-die activists who insist we should be free to kill ourselves whenever our lives are “complete.”
They have fallen victim, in critics’ eyes, to a kind of suicide contagion.
Statistics suggest these critics have a point.
In 2001, the Netherlands became the first country in the world to make euthanasia legal. Since then, the number of people who increasingly choose to die is startling. ”
If your life is so unbearable (as my niece “thought” her life was) that you cannot stand to live another day, you can end your life. There are multiple ways you can do this without engaging the legal approval of the state. What is anomalous should remain anomalous, not legal.
Thanks for your reply and the references. Peace to you!
And you.
Studies of people who survived jumping off the Golden Gate bridge report regretting it as soon as they jumped.
One reason the suicide rate is so high in the USA, guns are so efficient at killing people, they don’t have a chance to survive and recover.
https://www.cnn.com/2023/11/19/us/golden-gate-bridge-suicide-safety-net/index.html#:~:text=Hines%20is%20one%20of%2039,Francisco%20on%20April%205%2C%202023.
Doug, this reminds me of Eric Steel’s movie, The Bridge. Have you seen it? If not, I can tell you that it is both riveting and disturbing.
https://www.thebridge-themovie.com/
Not about mental illness, but assisted suicide is a somewhat active topic in Hungary now, because a constitutional lawyer who is dying in ALS started a fight for legalization. It (the fight for legalization) is nearing its end tough, because he has difficulties to even talk by now. And of course Hell freezes over before our government even considers this, they refused to even discuss it.
I think that people of sound mind should be able to decide what to do with their lives—including ending them. Some methods are better than others, however, and stepping in front of a subway train could entail lawsuits (and an ugly mess). Better to choose a different option.
One issue at stake is whether the person really is of sound mind. People who are severely mentally ill are, by definition, mentally disabled. But if the person really is capable of sound reasoning, then I think that the option of assisted death should be available. The rules regarding people who are severely mentally ill should perhaps be different than the rules for those who are mentally sound.
Finally, I can’t help wondering if there is an analogy here with the issue of gender affirming care. Many people seeking such care would probably be better off without it, but once transition takes place it is often irreversible. Yet, the gender-affirming care advocates say that people who want the treatment should be able to get it. The result has been—and continues to be—that more people are transitioning than should be.
I can picture a similar situation with assisted death. The big difference is that gender-affirming care advocates (at least sometimes) actively encourage patients to transition. In principle, those assisting with suicides would *not* be actively encouraging suicide, but would be following the appropriate protocols. That said, there *could* be some practitioners around who would do the wrong thing, which is a possibility that would need active monitoring. I suppose that this problem applies to all practitioners who offer assisted suicide, not just to those seeking it because of mental illness.
One thing that is being discussed here in Canada is the “advanced request”. In other words, if you believe you will in the future be a candidate for assisted death but will be unable to ask for it, you could file an advanced request, which somebody else could enforce on your behalf when the time comes. Here’s a link with a better explanation:
https://www.dyingwithdignity.ca/advocacy/allow-advance-requests-now/
Another issue is that medical institutions aren’t required to assist you with aid in dying, so if you’re in one of them then you have to get out of bed and go somewhere else to die.
Fascinating. The advance request is an interesting concept, much like an advance directive, or even part of one.
You forgot the reason to object to assisted dying the I find the most compelling. And I think it’s not a coincidence that this comes from a nation that places “freedom” above anything, but is so an individualistic society that always forgets to account for the fact that FORMAL freedom (“on paper”) is not the same thing as having the MATERIAL CONDITIONS to really exercise the choice freely.
Of course I write from a country that deems illegal selling organs, and you don’t see a problem there either. But THERE IS a problem. The problem is that the rich get to buy them, and the poor are FORCED to sell.
I already see your objection: isn’t it still better for them to have this option? No, it isn’t. It’s just a hypocritical defense of privilege. They wouldn’t choose so if they had other means. So there are two bad consequences:
1) this disincentivizes the society to find other measures to relieve their condition
2) this put pressure on other people, who wouldn’t choose so, but now live in a society where this affects them too (it’s the same as people accepting lower wages, this is a problem for everybody).
The same kind of reasoning applies to assisted dying.
I have always thought people should be free to end their life when they want, but then, as another reader as already commented, I was always in favour of people getting sex reassignment surgeries too, and we now are in a mess caused by ideology, social contagion, and lack of safeguards.
We already have many examples of things gone wrong where assisted dying is legal (Canada above all).
A recent column in the Times explicitly argued in favour of terminating “unproductive” elders. A canadian poll found that a majority of people is in favour of terminating poors and houseless people (not kidding!).
And there are many personal accounts of people who asked for health care (you know, those civilized societies where the State pays for it), were DENIED CARE and OFFERED ASSISTED DYING INSTEAD.
If you don’t find that problematic, I don’t know what evidence could convince you.
Please have a read to these:
https://www.theguardian.com/commentisfree/2024/apr/07/conflicted-legalising-assisted-dying-sonia-sodha
https://thecritic.co.uk/matthew-parris-and-the-illusion-of-independence/
(archived here https://archive.is/CbeNO)
https://www.compactmag.com/article/assisted-dying-isnt-freedom/
https://www.spiked-online.com/2024/03/28/now-canada-is-euthanising-autistic-people/
https://nationalpost.com/news/canada/canada-maid-assisted-suicide-homeless
As I’ve written, and you’ve neglected to check, there are problems with selling organs, but there’s a compelling case to be made for allowing it with restrictions. As far as the “slipperly slope argument,” that is worth sonsidering, but there are regulations that can elimionate that.
By the way, your email is rather rude, so please try to be more civil.
I beg your pardon, I’m not a native english speaker.
I can see rudeness in my critique of the individualistic mentality and of the US health care but I fail to see what I did wrong in the e-mail, I just tried to get straight to the point in order to not waste your time. Please forgive me if I did something (else) wrong.
Please, have a look at the articles I linked, they explain better than I can.
(I haven’t found references to organ selling in this post. I’m reading you since a couple of months, I admittedly didn’t check before and I still think there wasn’t a need to do it, since it’s not the main focus and it seems to me I correctly guessed your position. Now I found this https://whyevolutionistrue.com/2018/03/17/social-justice-warrior-would-rather-let-someone-die-than-donate-her-organs-because-they-might-go-to-rich-or-overeducated-people/
I’m still not convinced, and still think it’s an individualistic stance which conveniently discards the power differences. I suspect mine is a pretty common view in Europe.)
I did not find your post rude. Just a little blunt.
Chill Jerry.
I think that you’re making a distinction between choosing assisted death as an option *in principle* vs. it being an option *in practice.* In practice, I believe you are arguing, the risk is that economic and other societal conditions might end up making the choice of assisted death less of a choice than it should be in principle—in other words, that societal conditions might push people toward assisted death when in fact that is not what they want. Rather, lack of other options combined with societal pressure might push people into a death that can be prevented. That would certainly be one of the factors that regulation would need to guard against.
Can regulations fail to protect people in certain cases? Probably yes. Regulations can fail. Would legalization of assisted death for mental health disability disincentivize efforts to identify other options? I don’t know, but perhaps not. My guess is that the need to find options for people who *do not* want to choose assisted death will remain strong.
… but only when they request it. So long as we maintain that principle, I don’t have a problem with what is happening in Canada or elsewhere (or indeed, with Matthew Parris’s column, which seems to have caused a kerfuffle).
“but only when they request it”
If it is really about requesting a service, then this service should be offered to every responsible adult, not just to people considered a burden on society.
Instead, we hear members of the majority say that it sould be offered and provided to vulnerable minorities.
But killing someone because you’ve deemed them useless is another thing from that person asking to end their life because they are in pain and distress that cannot be remedied. The choice is made by the person suffering and the legislation requires that avenues to relieve that suffering are already tried. This seems to me to be apples and oranges.
It seems to me I haven’t been able to explain myself clearly. Though I think there is abudant evidence slippery slope has ALREADY happened (otherwise we would be speaking only of fatal deseases and not of whatever reason a person can have), the objection doesn’t seem exactly that to me.
The problem is focusing only on the fact that a person asks access to assisted dying neglecting to account for the reason they do so. The fact a person says the choice is their doesn’t mean it is, even less it means they weren’t pressed, conditioned into that.
The problem is not “relatives killing their grandmothers”, this is an unfair characterization of the argument. The problem is grandmothers “choosing” to die because their health care costs too much and they don’t want to deprive their relatives of these money. “Choosing” to die because they see their life is a burden for those they love.
I quote some excerpts from the articles.
“A decade ago, I would have supported assisted dying out of a respect for personal autonomy and a desire to alleviate suffering. Today, I understand these objectives are not standalone but need to be weighed against the impact on those for whom an abstract liberal notion like autonomy is highly simplistic, and the state-sanctioned wrongful deaths that seem to me impossible to avoid (…)
There will be women who get a terminal diagnosis, whose partners have been emotionally abusive to them for years – telling them their life isn’t worth living – who will come under intolerable pressure to opt for assisted dying. How can we ignore that around a third of female suicides are thought to be related to intimate partner abuse? (…)
There are relatives who will find ways – perhaps quite subtly, even unintentionally – of hinting to people with a terminal diagnosis who need round-the-clock care that they should opt for assisted dying. How would that make you feel? Almost half of people who chose assisted death in Oregon in 2022 cited concern about being a burden. (…)
Then there is the internal pressure that arises from some feeling that they ought to do it to save relatives difficulty and financial consequences: where the right to die becomes the duty to die. That message will be reinforced at a societal level; Times columnist Matthew Parris recently argued in a widely condemned column that assisted dying could help address the cost of an ageing population; that there are those willing to be honest about this should give serious pause for thought. (…)
There have been reports of officials promoting assisted dying to people with disabilities applying for government assistance and medical professionals trying to coerce people into it” (Sonia Sodha, the Guardian)
No due process can catch this kind of things. These are structural problems, that are not solved by having double checks on clinicians and judges. I’m not so naive to believe we can achieve 100% success: of course any human things would have “false positive” and “false negatives”, which in this case mean people that want it not having access on one hand, and people being forced on the other. But the solution can only be cultural.
I think that the “gender affirmative” approach for gender distressed people, and the skyrocketing number of young people accessing irreversible treatment in these recent years, show that in this society is simply not possible to strike a just balance between these two type of “errors”. The balance weigh against vulnerable people that are induced to harm themselves.
In the long run, one can hope for a cultural change, but at the moment the only solution I would personally believe in is one that allows assisted dying only for terminal physical illnesses for adult mentally capable people.
I was the one characterizing the argument that way, not Diana, and you are misstating what I said. If you read what I said when I explained it, your scenario is irrelevant because of the strict regulations that all of us would put on the decision.
Yes, we know you want it only in cases of terminal physical diseases, but some of us disagree with you, and we can argue our position. And of course there will be problems but striking a balance is possible and has been done in the Netherlands and Switzerland. You may disagree with that, but you have made no convincing argument that there are terrible wrongs committed in countries like the Netherlands and Switzerland.
Please try to avoid overcommenting on this thread, especially if the comment are long, like this one.
OK, I’ll bite. Why is that a problem? (Presuming that they do genuinely feel that — which they indeed may — and it really is their choice.)
Spending vast resources on extending life of very low quality by a few months doesn’t seem all that sensible to me.
Thank you for the links. Canada is going too far IMO. They’re trying to make it more and more available. Where will it end?
And I feel Canada needs to go further and include medical assisted dying for those with mental illness. These arguments seem to be a weird slippery slope that I saw with gay marriage….where will end? Will people be able to marry their dogs? No. It doesn’t work that way.
By framing the illness as a mental one, rather than a purely physical one, the hurdle is, by default, did this person make their decision with lucidity? Did they have capacity?
Personally I am conflicted.
I’m not opposed to suicide, but I would dispute the claim that someone’s depression, say, is incurable. How do we know that? We can know when physical illness is terminal in many cases, but the causes of depression and the workings of the brain are still largely inscrutable.
What has she really tried to improve her mental situation? It’s possible that her depression is rooted in a deformation of the brain, but it’s also possible that she could be cured with a change to a more fulfilling lifestyle. Get out of the house and into nature. Get a dog. Get married and have a child. Has she tried such things, or does she just sit inside because she’s depressed? It can become a self-fulfilling prophesy.
In her case we might have a clue from the claim that she’s suffered depression “her whole life”, but I also wonder if that claim is true. Was she deeply depressed even as a small child? Or did it only start later, in her teenage years, say?
Overall, I don’t oppose suicide for mental pain, but I oppose justifying it with unknowable claims about the pain being incurable.
Adam, the word “unknowable” in your last sentence is the kicker. This goes back to the perhaps unsolvable mystery of qualia. The only person who can verify the mental pain is the one experiencing it. See my reply to Rosemary above. Though it sounds tautological, the very fact that someone took their own life to escape from their pain is ex post facto proof of how intolerable the pain was.
“Though it sounds tautological, the very fact that someone took their own life to escape from their pain is ex post facto proof of how intolerable the pain was.”
Stephen, I agree with this, 100%.
IMO, “I (or the state) forbid you from ending your life because I (or the state) know better than you” and “I (or the state) suggest you end your life because you’re old/disabled/poor” are just two sides of the same coin. It’s one party telling another party when it’s time, or not, to go.
So, IMO, the rule is simple: No one (or entity) gets to tell someone else how to deal with the “when” of the end of their own life.
+1
+1!
(To Stephen’s first tag off #10)
“Unknowable” is the “kicker”, indeed!
Some of us know.
If she’s tried all possible cures, and, as her doctors say, there is no hope for her, then I’d pronounce her incurable. Do you want to be the one to tell her to get out more and get married or have a kid? That, I think, is pretty arrogant (and somewhat sexist). She has tried what the doctors recommended. Remember, she has borderline personality disorder and autism, too.
So go to the Netherlands and give her a pep talk; maybe you can save her since the doctors can’t.
I’m on my way! 🙂
I said what I said as someone who was depressed for a few years, thought life was pointless, and even considered suicide. I don’t know her situation, but at least for me a big lifestyle change was what I needed. It’s easy to spiral downward in depression when you stay inside the house, especially if you’re usually there alone. And I know that when you’re depressed, being told to go outside and socially is not as easy as it sounds, because you may really, really not want to.
But now I’m married with beautiful children who bring me such joy that my old life is almost incomprehensible to me. I can only say that I was seeking the wrong things – things which may have sounded good to my younger self but never brought me fulfillment.
As I said, I don’t know her situation, and I don’t know what the doctors have suggested or how earnestly she really tried it, but I still hold that we don’t truly know her situation is incurable in the same way that we can know a cancer that has spread throughout the body is incurable. And in any case, perhaps it makes little difference to the argument for or against assisted suicide.
I think unbearable should be the standard. Not incurable. Such things cannot be determined from the outside looking in.
Here I agree with you (regardless of our mutual opinions of each other). Particularly about depression, I am worried that the suicide of people with depression, which used to be regarded as a worrying example of failure of medicine and a call for more research and care, is not being touted as the ultimate cure of depression.
I guess it’s not mutual, but my opinion of you is a good one. 🙂
Thank you very much! You once wrote a very sharp comment about me – now I suppose that it was not really your opinion but just emotionally expressed strong disagreement.
I am very glad that your life has turned to better.
When you’re treated for depression all these things are considered but honestly someone who is chronically depressed isn’t that way because they haven’t gone on enough walks in the forest. It comes across as very ableist and condescending to suggest such a thing. Sometimes nothing works. No medicine can cure you, no change in life can help you and this may come as a surprise but some women don’t want to have children and doing so for them makes it all that much worse.
+1
+!
Out of some curiosity, I looked up information about whether doctors ever, you know, assist the process on the down-low in places where assisted suicide is illegal. That apparently happens here and there and I am not too surprised.
In 1997, a doctor in Nova Scotia was charged with first-degree murder after a hospital physician colleague complained to the police that she had done exactly that. Pick your witnesses and assistants very carefully. We used to be taught in school that no physician in North America had ever been charged with a crime in the acceleration of the dying process. Not so any more.
The case never went to trial because a preliminary hearing (the very rough correlate of a grand jury in Canada but presided over by a judge, not a prosecutor) determined there was not enough evidence to make a conviction likely, even though that evidence included her administration of drugs of no value in pain relief, potassium chloride and nitroglycerin.
https://go.gale.com/ps/i.do?id=GALE%7CA106026702&sid=googleScholar&v=2.1&it=r&linkaccess=abs&issn=11928336&p=AONE&sw=w&userGroupName=anon%7Eb8b97f9b&aty=open-web-entry
This reference is paywalled but the Canadian Encylopedia has an entry on the case taken from a popular magazine.
I wonder whether the number of people choosing assisted suicide might ever reach a tipping point at which it became a societal norm—and expectation. Not that human beings ever pressure each other, be they loved ones or strangers. Not that governments and taxpayers would want to save money, with health expenses and existing government debts being what they are. Nor would family members want to preserve potential inheritances. And human beings never ostracize or morally condemn those who make different medical decisions. We always respect “My body, my choice.”
I mean, after all, when we learned that the COVID vaccines did not prevent transmission and were thus a choice about personal—versus community—wellbeing, then we treated the anti-vaxxers kindly, didn’t we? We didn’t come up with a dehumanizing term that blurred any nuance about why a given person might make the decision she did under the specific circumstances of her age, health history, and life. No, we didn’t do that; we didn’t insist that our choice should apply to everyone. Nor did we ostracize people, cutting off family members and long-time friends. Nobody was morally condemned. Nobody had their access to public facilities blocked. Nobody was barred from attending a university. Nobody took the public position that if unvaccinated people got sick with COVID, then they should be denied medical care rather than take up limited space and burden us with the costs. We never mandated vaccination anywhere. We never directed that people be vaccinated at threat of losing their jobs; and, of course, we never fired anyone who refused the shot. After all, their choices didn’t affect us personally; the vaccine didn’t prevent transmission, and our vaccines protected us. No, we would never interfere with nor dictate what another person does with his or her body.
I’m not saying that such things WOULD happen in the realm of assisted suicide, and I’m wary of slippery slope arguments because just about any possible future can be imagined. But we must always remain alert to the tensions that play out between individual choice and rights and the ways that groups of like-minded people can treat dissenters—especially if the group has power to enforce their will, power to declare whether you are fit to make sound decisions, power to declare your choice unsound because it is not their choice. Right now, the power remains with those who want to deny the choice to die. In the future, it could reside with those who want to “encourage” you to die. Tred cautiously.
There is another assertion often made by opponents of assisted dying, which is that once it becomes accepted in society, some family members will start to put pressure on their elderly relatives to volunteer for it, whether they are terminally ill or not. Despite anecdotal evidence, I am not aware of any serious study that has shown this to be a potential problem. So if there is really no evidence for it, it needs to be called out.
FWIW, I am in favour of complete autonomy for the individual. I am fortunate enough to have no serious illness or mental condition (not sure all my friends would agree about the latter…), and I think it would take an awful lot to make me prefer death to life. But I have considerable sympathy for those who don’t.
I dunno, if someone said to me, “you know Diana, you’ve lived long enough. Have you thought about suicide”? I might think “Well that one’s a bit of a jerk. Maybe I shouldn’t listen to them”. I would hope anyone else would feel the same. I just am not convinced that the elderly are going to opt for things because they are being pressured and there are laws around such things. I recognize there are power imbalances but there are protections agains elder abuse, etc.
I am in favor of people having the ability to end their own life when faced with a terminal illness or constant pain. I have concerns about how this can be legislated humanely as a general concern, and very much so once mental illness is included. As our medical care cost crisis worsens, some groups of people will be perceived as too expensive to maintain. Limits on who receives what type of medical care are inevitable. News reports of vulnerable people being coerced in order to take their money are not unusual. People with mental illness can be added to the physically disabled, powerless poor, and folks with dementia as hopeless cases who contribute nothing to society while placing an unjustifiable economic burden on “productive people” (taxpayers.) I am caught between wanting an enlightened, compassionate society that allows dignity in dying and my realistic fears that there have always been people willing to harm others for gain. How is this to be legislated with wisdom in a time when the US will have an authoritarian dictator wanna be on the presidential ballot?
One suggestion: start campaigning for Biden! 🙂
Yep!
My father chose assisted suicide when he had terminal (and incredibly painful) cancer. In his case this only reduced his life by a few weeks, but they would have been tormented weeks. No painkiller that leaves you conscious can help the pain.
A tiny bonus, was the whole family was able to gather on “the day” and say goodbye, then be together to support each other. Almost a pre-funeral.
Condolences, alexander. The mourning labor is very important, glad to learn that you and your family were able to do it together.
I add my condolences to Alexander. I also want to note that I added one argument that slipped my mind–the “slippery slope” argument–to the list of counterarguments to assisted dying for mental illness. I’ve put it as #5 at the top of the post.
I fully agree with Dr Coyne’s views, as expressed in the post. For reasons I won’t go into this is an emotional subject for me, though I will clarify that I too am NOT a candidate (though who knows what the future will bring).
Most of the objections to assisted suicide, apart from the God forbids it malarky, which fortunately no one here is pushing, seem to center around some formulation of the “slippery slope” problem, of which “it’s contagious” is a new iteration. Some seem to take this all the way to “it will blur the line between life and death”. I am a little surprised at these foreboding views of a dystopian future where death will be encouraged (if not mandated) for certain people. Not that I have an particularly optimistic outlook on social patterns, but I think it’s a distraction from what is an important issue in the present.
Without doubt, there are practical concerns about how assisted suicide is implemented, and of course it is possible that there could be instances of abuse. But there are many things in our society of which the same could be said, and we find a way to manage despite this. As others have stated, there are ways to regulate the practice, and while writing the rules may be challenging, this is the only humane path forward. We have, I do believe, emerged from the Middle Ages. Of course we’re humans, so these rules will not in all instances be interpreted or applied perfectly, but this cannot be a reason for banning the practice entirely. We cannot accept the cruel alternative of enforced suffering.
I concede that mental health is harder, as I have always believed that the knowing consent of the patient is a fundamental requirement. Where there is concern–legitimate concern, not a fabricated excuse–as to whether that consent is valid, things get difficult. But with proper guardrails in place, I support the right of persons affected by this form of suffering to determine their own fate.
Yes, life is precious. But that doesn’t give anyone the right to force other people to live lives they don’t want to. I personally find the idea that someone else can tell me that I cannot end my life if I so choose to be an outrageous theft of my personal integrity. I am shocked when people of intelligence and insight take the position that it cannot be permitted. Playing god after all, are we, with someone else’s life?
No one should ever step in front of a train. Where appropriate, there must be a humane alternative for such people. Outlawing that alternative is barbarism.
Well said and I agree that the legislation must be crafted and questions asked but some of the arguments against medically assisted end of life seemed inconsistent when it comes to mental health, for instance the not being able to consent but there are brain conditions that affect cognition, including dementia, that can impede thought that are currently allowed. I get that consent is important but let’s be clear that there seems to be a bias when it comes to mental illness (of which there are many with various degrees of lucidity) & I believe that bias stems from the dualism that has a strong grip on our intuitions.
I actually find it comforting that if things got bad for me, I have the choice of medical assistance to end my life – doing it on your own can be very inconsistent in the results and much more traumatizing for everyone around you & if they help you then they can be sent to jail and their life ruined.
Very well stated.
Regarding slippery slopes: “Yes, this is a danger, though one that can be ameliorated with sufficient stringent vetting laws.”
I’m glad that Jerry deems the slippery slope argument worth considering. I would add one more consideration. When it comes to suicide, assisted or not, we previously lived in a culture of prohibition. We are moving to a culture of restraint. One day, the restraint may give way to a culture of acceptance—without reticence. Acceptance can morph to expectation. If such a society ever comes about, your laws and regulations will not protect you. The laws follow culture, they do not drive it.
We currently see an assault on various laws, regulations, and constitutional protections that govern social issues of all sorts. Our generation once thought these issues settled, or at least tolerably so. Many in the younger generations disagree.
I live in France, where the government is proposing legislation to allow some form of “aide à mourir” (help with dying). Among other things, they are insisting that the person requesting it be in good mental health. My mother, who suffered from extreme Alzheimer disease, reached the point where she did not recognize her own house or husband, and even ran out into the street in her nightgown at least one night, crying for help. I do not want to wind up like that. So I am extremely leery of insisting upon the person’s being in their right mind when that no longer exists.
It still seems to me that 95% of objections to assisted suicide or euthanasia are due to religion, from which we still have not yet liberated ourselves after millennia of trying. (Think Epicurus.)
Yes, but some mental illnesses don’t take away the “right mind” that can weigh the advantages and disadvantages of assisted dying. I believe that the Dutch woman highlighted in this article is certainly compos mentis enough to decide if she wants to die. “Right mind” for such cases means, “able to make a rational decision after assessing the consequenes.”
My main argument is that we put pets ‘to sleep’ when they are suffering without prospect of a cure and consider that a kindness. To keep people suffering without a prospect of a cure is an unkindness – and done for no significant reason.
I agree completely. The real criterion should be something along the lines of “Is the person still getting something positive out of life?”, but that is difficult to define.
A most excellent, thoughtful, edifying discussion. A reason I come to WEIT.
Thank you.
Indeed!
Jerry’s question narrowly focused on the morality of assisted suicide for, specifically, people with mental illness.
I think we all agree that mentally competent adults have a moral right to kill themselves and, I thought (and still think pending being shown to be wrong), that it is not illegal in most of the world to make the attempt.
The phrasing of the question implies that the morality of requesting assistance with one’s suicide for intractable painful or otherwise intolerable physical illnesses — the illness no longer has to be progressing inexorably toward death in Canada –, is settled. Perhaps it is. The only question seems to be if it’s also moral to want help ending your life for mental illness. By the principle of autonomy it seems that you don’t need to offer a reason why you want to die, only that you do, so that the machinery of the assistance mechanism can be activated. So asking for assistance in killing yourself for mental reasons doesn’t seem to be any different, morally, from requesting it for physical illness reasons or, indeed, for no reason at all.
But wait. Assisted suicide requires the cooperation of an assistant who in most cases must carry out the planned deliberate killing of you. Murdering you in other words. If the assistant merely provides you with the means, which you use (or not) by your own hand at a time of your choosing, only that is assisted suicide (which I think is uncommon in Canada, because unreliable and there is the risk that lethal drugs attractive for abuse will be diverted to the street if not used as intended.) So the soon-to-be deceased have transferred in a moral sense the responsibility (and any culpability) for her wish to die to someone else who actually does the deed for her and who will be around to bear the legal and moral consequences of her decision.
This I think is where the real moral conundrum of consensual murder (or assisted suicide) arises. The train driver who kills a person on the tracks is morally blameless (and indeed does suffer a moral transgression by the hand of the suicide, as J Stevens implies) but the agent who causes or collaborates in the death is not blameless just because the suicide consented. The law is clear on that. So while it is moral (and presumably legal) to ask for assistance in killing yourself (or to do the whole job for you), it is a morally and legally fraught decision on the part of the assistant or murderer to acquiesce in it. With a wave of its hand the law writes an exemption for murder (or assistance with suicide) carried out by physicians working in the context of medical practice, which it did in Canada only because the Supreme Court decided that doctors ought not to be punished for deliberately killing people who wanted it. It was consumer demand, not moral reasoning that led to Canada’s euthanasia law.
This leads to the final, and unsettled, moral dimension of the question: Since there is a right to request your own murder (or assistance in suicide), is there a corresponding obligation on the part of the designated assistant to comply? Or is there only a promise of freedom from prosecution for murder if the medically qualified assistant agrees to do it? The question is pointed in Canada because I think a lot of doctors were taken aback by how quickly (i.e., immediately) the permission to murder on request became framed by licensing regulators as professional misconduct if you refused to do it…or make a “meaningful referral” for all who “qualify.”
This is where the moral differences between reasonably foreseeable death from physical illness (the original law) and mental illness become acute. A doctor comfortable with killing a suffering patient soon to die from cancer might feel less comfortable, off soundings we might say, with killing a chronically depressed person with nothing else wrong with her…and who might well eventually change her mind, as we know most people who survive unassisted suicide attempts do. Yet the regulator would insist he must comply with either request if euthanasia for mental illness becomes law. But does the doctor have the right to refuse the one, on the moral grounds of duty to prevent death from suicide where he can, but not the other? Or refuse both for that matter?
In Switzerland, the medical person prepares the brew, but you have to drink it by your own means. That is assisted suicide, not murder. Curiously, in Belgium, it’s the doctor who must administer the fatal injection.
Why not make assisted dying for any reason be permitted after a certain age? I am 89, in control of my life and actions, rational, emotionally stable but depressed from losing my husband of 62 years. I can barely walk, live alone, have very few friends, cannot go out to movies or museums or go on bird walks, have no interest in cooking, physically handicapped and barely able to go up or down stairs, cannot travel, am extremely lonely. There is nothing for me to look forward to. I am both wracked with anxiety when I wake up, and bored and have almost no company to talk to. I am NOT suicidal! I wish I were. But I would welcome assisted dying. My life in the real sense is over. Why cant my rational
honest desire to move on after a long life be fulfilled?That would be giving ME
control over my life, autonomy. MY life doesnt have anything to do with other
peoples’ so-called respect for life. It is MY life and my respect for it that counts. I am a mature rational being confined to a small space and deprived of all the things that make life worthwhile. I think my wishes should be respected by society.
i am very touched by your words and I understand that you don’t want to commit suicide but rather would like to go to sleep and never wake up again. thats a big difference!
I wish you all the best.
Hi Lorna. I read your comment last night and it’s still affecting me. First I want to say I’m sorry you’ve lost your husband of 62 years! I don’t know how couples who’ve shared a lifetime together manage to go on once their partner has passed. You’ve described your daily life with such candor and lack of sentimentality… It’s palpable. What strikes me personally about it is, were one to remove the age and physical handicap portion of your account, how common such isolation and deprivation of social stimulation is in today’s American society. There are many people who have no one to go to movies, museums, and bird walks with. Or, no money or transportation to get there. I’m struck by the commonalities of old age and poverty. I know so many people who are 20-30 years younger than you who would describe their lives just as you’ve described yours. It’s dismal. I find myself wondering if, for someone like yourself who once had such a full and active life, if the pain wouldn’t indeed become unbearable. I very much resonate with your statement, “MY life doesn’t have anything to do with other peoples’ so-called respect for life. It is MY life and my respect for it that counts.”
Many thanks for your compassion and understanding. The past six years have been hell to one degree or another. I have always been well adjusted emotionally, rational, responsible….but my husband’s death shattered my emotional condition. This persists when I am alone but luckily if I have visitors and can talk to people, I feel OK! A less stable person would have gone crazy by now. The strange thing is that my grief is greater now than in the first two or three years following his death. Maybe I was in denial or disbelief. At some point I thought he was watching me from above (and I am an atheist). I also wonder how other people in my position or worse survive. Many dont. Many cant. My brain seems to be able to bear up. Thanks so much for writing.
At least a 28 year old’s assisted suicide has nothing to do with the subversive religious cult called communism.
#degrowth
#death cult
#agitprop
#ideological remoulding
#social emotional learning suicide surveys
#multi tiered system of support (MTSS)
#psychodata
I’m including a response to a comment above as an independent comment:
++++++++++++++++++++++++++++++++++++++++++++++
I remain unconvinced that legalizing suicide for humans with psychological issues (assisted dying in the case of emotional distress) will lead to a “better world” for all.
My niece took her life in 2022. I don’t judge her for her decision, never will, and will continue to grieve her loss; should her decision (at 19+) been legal and sanctioned by the state. I say vehemently – No. Suicide should remain an anomaly to *life*.
Yes, death is a relief from suffering, but the legalization of death in the form of assisted dying (particularly in the case of emotional distress) normalizes a way out.
It’s not a giant intellectual leap to “see” that the end-game of normalizing mental illness via legal avenues (currently sweeping the west – WEIT writes about it implicitly and explicitly), can and does lead to normalizing suicide; leading to more suicides; and -clearly- there are unforeseen consequences to legalizing suicide (see below) besides the alleviation of suffering.
The west appears to be obsessed with erasing all forms of pain, suffering, discipline, and long-term thinking/solutions from its cultural zeitgeist.
The author of the FP piece cited by WEIT (Rupa Subramanya) discussed her findings with Megyn Kelly, (below) her research suggests that in every region/state/country where assisted dying is legal, suicide (outside the purview of *assisted suicide*) has also risen. A form of ‘suicide contagion’.
“Disturbing Rise of Young People Dying By Suicide… Including Assisted Suicide, with Rupa Subramanya”
https://youtu.be/yYiIxCspsfM?si=XOz-YfWe4iz6-SaB
Also, from the article: https://www.thefp.com/p/im-28-and-im-scheduled-to-die
“Theo Boer, a healthcare ethics professor at Protestant Theological University in Groningen, served for a decade on a euthanasia review board in the Netherlands. “I entered the review committee in 2005, and I was there until 2014,” Boer told me. “In those years, I saw the Dutch euthanasia practice evolve from death being a last resort to death being a default option.” He ultimately resigned.
Boer had in mind people like Zoraya ter Beek—who, critics argue, have been tacitly encouraged to kill themselves by laws that destigmatize suicide, a social media culture that glamorizes it, and radical right-to-die activists who insist we should be free to kill ourselves whenever our lives are “complete.”
They have fallen victim, in critics’ eyes, to a kind of suicide contagion.
Statistics suggest these critics have a point.
In 2001, the Netherlands became the first country in the world to make euthanasia legal. Since then, the number of people who increasingly choose to die is startling. ”
If your life is so unbearable (as my niece “thought” her life was) that you cannot stand to live another day, you can end your life. There are multiple ways you can do this without engaging the legal approval of the state. What is anomalous should remain anomalous, not legal.
Thankfully most people are incapable of committing suicide. I am not mentally disturbed in any sense. I am completely rational in not wanting to continue living. Modern medicine has allowed us to live much too long. With assisted dying, one respects the individual’s choice. Assistance is needed precisely because mentally stable rational people are not able to. it is minimal and usually the person presses the button. I find a lack of empathy more disturbing. If we value individuals, then we should accept their decision. Society has nothing to say about it.
We can agree to disagree. With empathy. It’s a fine balance (not much daylight) between individual rights and corresponding societal impacts (in this case of legalizing suicide or legally assisted death).
My niece took her life in 2022. She was 19. Not 91. She was in a highly distressed state. I wouldn’t call that a ‘rational’ state. One can be in such a state for year, two years or all one’s life. So far, the data shows (see my comment) that legalizing assisted dying amplifies suicide; meaning a “suicide contagion” results. Young people don’t have the maturity OR experience to reason as adults do. Their brains are not quite formed and social media (where many young people live their lives) leans to glorifying death.
It’s quite possible that new data and analysis may demonstrate stability or a decrease in suicides where assisted dying is legal; so far it hasn’t, as of today, the reverse is true. I am open to changing my mind if and when the data shows otherwise.
I do value individuals. Not every decision made by every individuals is valuable or moral or worthy of emulation. Individual rights and societal stability have to be balanced.
I am not without empathy. I reject the implication.
Be blessed.
Very well said, Ms. Salzman. It is disturbing how the claim of some sort of social imperative is used to deny individuals the most basic right anyone can possibly have. Compassion for the suffering is, or should be, a paramount social concern, but somehow this gets turned on its head.
I hope that the rest of your life, for however long it continues, will be as peaceful and pleasant as possible.
As a doctor, I once swore to do no harm. And that’s where I see the problem: sometimes the line between helping and harming is very small.
In Austria you need, among other things, confirmation from a psychiatrist that you are in full possession of your mental health. What about mentally ill people? and even though I tend to be in favor of assisted suicide, the problem is currently not solvable for me.
At first I thought…somebody stop this poor woman, she’s only 28! But then, I thought of my own decision to seriously consider ending my life at 60. I’m 48, and to be frank the only things that keep me going are a small number of people that currently either depend on me or may be seriously traumatized by my suicide. But in 12 years or so, those folks will either no longer be dependents, or will be dead themselves.
60 years is plenty for those of us who never have really felt comfortable in their own skin. Some people love life, and good on them. That’s just not me, and never really has been.
I never gave my consent to be born so I’m not sure why I have to cling on for as long as possible. In fact, it gives me a sense of urgency and purpose to have nigh more than a decade left.