In 2023, Tennessee passed a bill to restrict access of minors to “affirmative care”, though only minors who wanted blockers or hormones to assume the identity of his/her non-natal sex or to relieve gender dysphoria. Tennessee is now one of 15 states that has passed laws restricting affirmative care. Note, though, that hormones and blockers may, under that law, be used to treat other disorders (also called “differences”) of sex determination {DSDs).
Click title to read the bill. In it, “minor” refers to “an individual under 18 years of age”

From the bill:
The legislature determines that medical procedures that alter a minor’s hormonal balance, remove a minor’s sex organs, or otherwise change a minor’s physical appearance are harmful to a minor when these medical procedures are performed for the purpose of enabling a minor to identify with, or live as, a purported identity inconsistent with the minor’s sex or treating purported discomfort or distress from a discordance between the minor’s sex and asserted identity. These procedures can lead to the minor becoming irreversibly sterile, having increased risk of disease and illness, or suffering from adverse and sometimes fatal psychological consequences. Moreover, the legislature finds it likely that not all harmful effects associated with these types of medical procedures when performed on a minor are yet fully known, as many of these procedures, when performed on a minor for such purposes, are experimental in nature and not supported by high-quality, long-term medical studies.
The bill does not ban that aspect of “affirmative care” that involves psychological affirmation of a minor’s desires; what is banned is solely medical treatment given to minors. (I do think that good psychological treatment doesn’t have an aim at the outset, though, so “affirmative psychology” seems counterproductive).
But when you turn 18 in Tennessee, you can have all the hormones you want, though puberty blockers are by that point superfluous.
Yesterday, the U.S. Supreme Court upheld the law by a vote of 6-3—the ideological vote that we liberals are used to. There are long concurrences by Judges Alito (22 pages), Barrett (11 pages) and Thomas (23 pages), and dissents by Sotomayor (31 pages) and Kagan (2 pages). Click to see the decision:

And the end of the decision:

The Supreme Court decision reprised the Tennesse law:
In 2023, Tennessee joined the growing number of States restricting sex transition treatments for minors by enacting the Prohibition on Medical Procedures Performed on Minors Related to Sexual Identity, Senate Bill 1 (SB1). SB1 prohibits healthcare providers from prescribing, administering, or dispensing puberty blockers or hormones to any minor for the purpose of (1) enabling the minor to identify with, or live as, a purported identity inconsistent with the minor’s biological sex, or (2) treating purported discomfort or distress from a discordance between the minor’s biological sex and asserted identity. At the same time, SB1 permits a healthcare provider to administer puberty blockers or hormones to treat a minor’s congenital defect, precocious puberty, disease, or physical injury.
The National Law Review summarizes the decision and discusses its basis and what it did not address (click to read):

An excerpt:
In a 6-3 opinion authored by Chief Justice John Roberts, the Court in Skrmetti affirmed the U.S. Court of Appeals for the Sixth Circuit,[1] which held in September 2023 that (1) the Tennessee law does not discriminate on the basis of sex for purposes of equal protection, and (2) that it was subject only to rational basis review.
“SB1 does not classify on any bases that warrant heightened review,” the Supreme Court wrote. It concluded that the Tennessee law incorporates only two classifications: (1) age (allowing certain medical treatments for adults but not minors), and (2) medical use (allowing puberty blockers for minors for some conditions but not others). These two classifications warranted only rational basis review, the Court said.
And the Court dodged the question of whether transgender status should be considered a protected class equivalent to race or gender. “This case, in any event, does not raise that question because SB1 does not classify on transgender status.”
That’s a serious issue, for if transgender status is a protected class, the whole game changes. That doesn’t mean, though, that gender-dyphoric minors will immediately be allowed medical “affirmative care.” It goes on:
. . . The decision marks the first time the Supreme Court considered the application of the Equal Protection Clause to transgender youth, despite the decision skirting the question of whether transgender status should be considered a protected class.
The decision has broad implications, although many legal issues in this area remain unresolved.
Those unresolved issues are said to involve the right to privacy, parents’ rights, statutory discrimination analysis, impact of state constitutional arguments, and tension with state laws on gender identity. The upshot, it seems to me, is that the Court decided that the Tennessee law, because it didn’t discriminate on the basis of sex (both male and females with gender dysphoria are equally subject to Tennessee’s ban), was constitutional on those grounds. But that still leaves the issue of whether “transgender status” or “having gender dysphoria” counts as being a member of a protected class. If that proves to be the case in further legal wrangling, then affirmative medical care may be permitted.
I am not sure how this affects the 25 other states that do not have laws against medical affirmative care; those states have not passed bills banning it (or, presumably, allowing it) that can be adjudicated at the nation’s highest court. (I may be wrong here, so readers who know are welcome to correct me.)
Some of the mainstream media are couching this as a “setback for transgender rights”, but some of us would argue that there is not a “right” for minor who wishes to have surgery and/or hormone treatments aimed at making them resemble members of their non-natal sex should be able to freely get such treatments.
Here are two articles explicitly endorsing such a “right”:
From the Associated Press:


There was an NPR article called “Battle over rights of trans children is up at the Supreme Court,” but it has now changed the title (!). It does still assert the “rights” in one paragraph:
Front and center at the Supreme Court on Wednesday is the battle over the rights of transgender children. At issue is a state law in Tennessee that blocks minors from accessing gender-affirming care in the state.
I don’t want to scour all the news for similar statements, though, because I don’t believe there’s any “right” of minors to affirmative medical care beyond psychological treatment; there’s certainly no right in the Constitution or—in my view—ethics to have parts of your body cut off or hormones injected into you, particularly when the vast majority of minors experiencing gender dysphoria will resolve as being gay children who don’t need this kind of medical care (especially unproven blockers, who are banned for minors in some European countries).
Emily Yoffe, whose writings I’ve always found pretty sensible, agrees with me, and published the article below in the Free Press (archived here):


Some excerpts from Yoffe’s piece (bolding is mine):
The Court’s ruling is narrow; it says that a state has the right to regulate the practice. States, mostly blue, that still allow youth gender transition aren’t affected. But the decision will likely lend weight to the arguments of people who want to end the practice nationwide. And it will likely help the legal efforts by “detransitioners”—that is, young people who say they were pressured into life-altering treatments they now regret—to get compensation. Surely more such lawsuits will now be filed. Gender transition clinics will likely be under far more scrutiny: This Free Press story describes the cases of two such young women who were given prescriptions for testosterone after about a 30-minute appointment at Planned Parenthood.
Children who express gender distress often suffer from a host of other medical and psychological issues, such as autism, ADHD, depression, or anxiety, or have experienced various traumas. But to the gender doctors in their lucrative new clinics, there was only one answer to such childhood troubles: gender transition. This usually meant medically blocking a child’s normal puberty, then putting that patient on opposite-sex hormones: testosterone for girls, estrogen for boys. Sometimes complicated and painful surgeries were undertaken to try to create new genitals. Thousands of teenage girls, and some not even teenagers, have received double mastectomies, known euphemistically as “top surgery”—a surgical intervention normally reserved to treat breast cancer.
In the U.S., gender-distressed children and their parents were told that without the swift intervention of these radical treatments, the children were likely to commit suicide. It became a cliché for the reluctant parents of girls seeking to transition to be asked by the gender provider, “Would you rather have a live son or a dead daughter?” (And vice versa for parents of boys.)
The clinicians assured parents there was robust evidence underlying their interventions, but this was false. During the oral argument in the case, Chase Strangio, the lawyer for the ACLU, arguing to overturn Tennessee’s ban, was forced to acknowledge to Justice Samuel Alito that “completed suicide, thankfully and admittedly, is rare.”
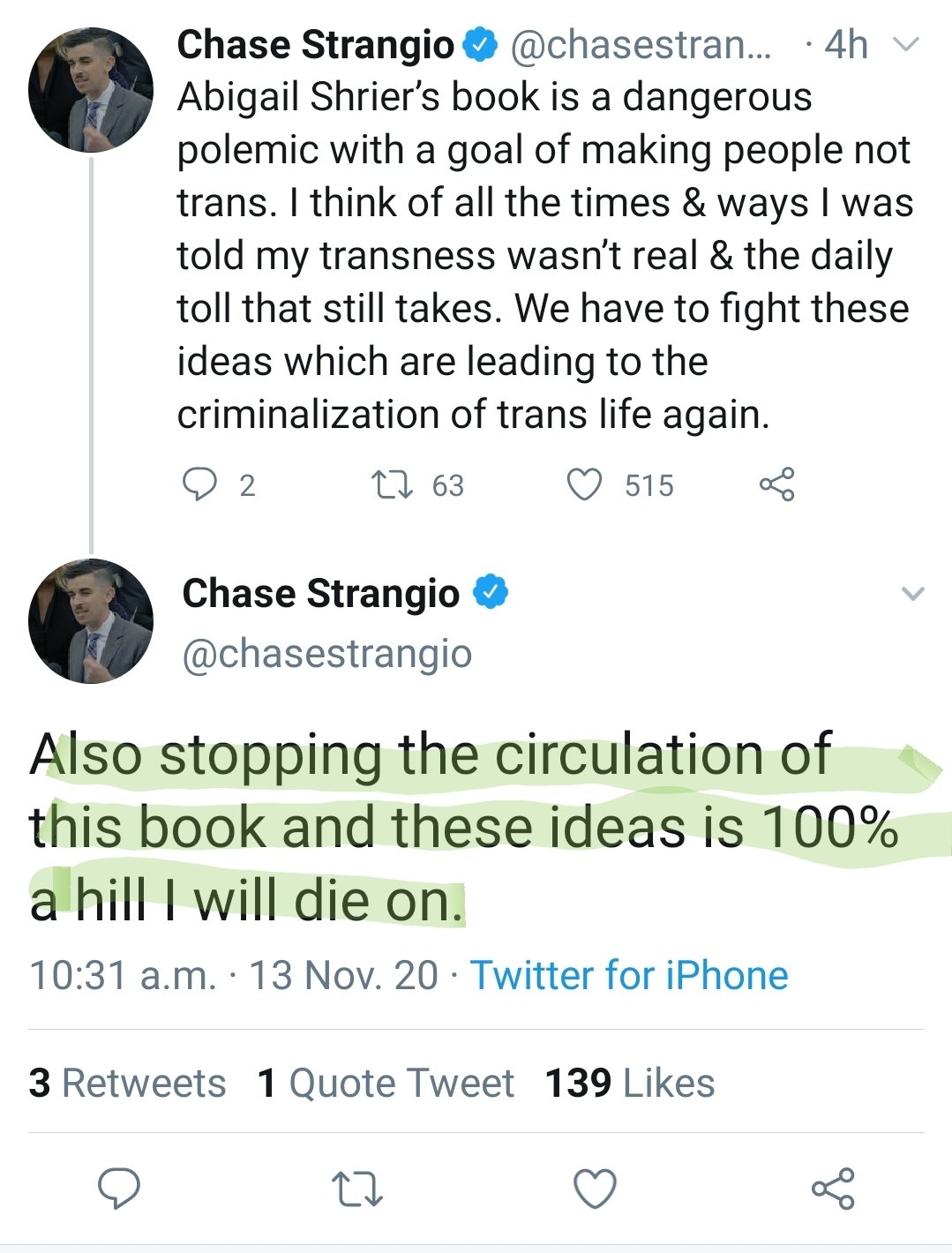
I would have guessed that Strangio would be in there argue for surgery and hormones; he was, after all, the ACLU lawyer who argued for banning Abigail Shrier’s book on rapid-onset gender dyphoria, often triggered by social pressure. (Strangio is also a trans-identified female.) In the end, Shrier was right. Shame on Strangio and the ACLU:
More from Yoffe:
. . . . The Court’s ruling notwithstanding, the U.S. medical establishment remains firmly behind the practice. Compare that to England, where a rigorous and independent report, the Cass Review, concluded that the evidence for pediatric transition is “remarkably weak.” Finland, Norway, and Sweden are among the other Western nations that have joined the UK in moving away from this treatment.
It is widely observed that the vast majority of young people with gender dysphoria—even those whose distress is “consistent, insistent, and persistent”—when allowed to go through normal puberty, come to accept their biological sex. (And there is no way to identify the very small number of children who will go on to experience lifelong gender distress.) Many of these children turn out to be gay, which is why a rising number of gay adults and gay-rights advocates have become alarmed that the transgender movement is medically transitioning gay kids. They argue that this movement has, intentionally or not, reified homophobic tropes.
I especially agree with the last paragraph below. In the future, I think medical gender-affirmative cafe will, along with our poor treatment of farm animals, be seen as practicers that were immoral in their time, but widely practiced:
Critics of the Supreme Court decision will argue that our major medical associations, from the American Academy of Pediatrics, to the American Medical Association, to the Endocrine Society, have all given support to this new branch of medicine. This is true. It is also true that these organizations or similar ones once supported lobotomies and eugenics. Just as that is a source of shame today, it is to be hoped that their vehement support of medically transitioning vulnerable young people will be a source of shame in the future. These medical societies have failed in their most basic duty of care to their patients by embracing a model that has so little evidence and such profound lifetime consequences.
When the history of this era is written, historians will have to explain how transgender activists so quickly took over institutions, and were able to so successfully threaten the social and work lives of those who objected. We are confident that historians will also remember those courageous individuals who, at the risk of professional and personal ruin, did so anyway.
But over at the Freedom From Religion Foundation, which now comprises a group of Chase Strangio clones, they’re proclaiming first that affirmative care is in general a salubrious way to address gender dysphoria, but also that affirmative care is “religious dogma.” That characterization is palpably ridiculous, meant as a way for the FFRF to pretend that its “progressive” politics are fully in line with its mission to keep church and state separate. But many atheists like me object to affirmative care. It is the FFRF’s deliberate conflation of progressive politics with church-state separation that I objected to, and this ultimately wound up with my resigning (along with Richard Dawkins and Steve Pinker) from the FFRF’s honorary board. Click below to read:

Note that the FFRF again speaks of transgender minors’ “rights”:
The Freedom From Religion Foundation lambastes today’s U.S. Supreme Court ruling upholding Tennessee’s cruel and unconstitutional ban on gender-affirming care for minors. This decision is a major blow to science-based medicine and the rights of parents and transgender youth.
, , , , Despite the hostile narrative surrounding transgender health care that the Supreme Court is furthering in its decision, the gender-affirming-care model is safe, effective and supported by every major medical organization, including the American Medical Association, the American Psychiatric Association, the American Psychological Association, the American Academy of Pediatrics and the American Academy of Child and Adolescent Psychiatry. These secular scientific organizations prioritize the safety and health of patients, not religious dogma.
The Freedom From Religion Foundation stands firmly with the transgender community, with parents, and with the medical professionals who follow science and ethics — not narrow sectarian belief — in providing care. FFRF will continue to educate about the harm these theocratic assaults are doing to civil liberties, bodily autonomy and the wall of separation between religion and government.
When the FFRF proclaims gender-affirming “model” as “safe, effective, and supported by every major medical association,” they of course neglect the fact that gender-affirming care is not seen that way in Europe, where it’s either banned or considered as experimental. And of course most gender-dysphoric minors who go through normal puberty don’t really need this care, as most turn out to be gay. No hormones or excising of body parts required. Affirmative treatment, as you may know, usually sterilizes its recipients, and, further, many of them will never have an orgasm after transitioning.
People like those in the FFRF are acting like this is the end of gender-affirmative care in America. I wish it were, and that treatment for dysphoria was limited to those over 18 (on same days I think 21). But in half of our states, hormones and surgery are still allowed, and there are no bans to be overturned. I think that such states are making a mistake treating youths who haven’t attained maturity as having the ability to make their full medical decisions, like catering to a minor who doesn’t like their left leg and wants it cut off. The “right” to make such decisions should not be given to minors, or even their parents or doctors—not until youths come of age.
This viewpoint may be seen as transphobic, but I firmly reject that adjective. After all, it’s not seen as transphobic in the UK, Sweden, Finland, or Denmark, which have severe restrictions on affirmative care. And in the future, those who defend this rush to cut and inject hormones will, I think, be seen as misguided or even barbaric.
As an illustration of poor the evidence for puberty blockers is, here’s Jesse Singal’s substack giving a critique of the recent Olson-Kennedy et al paper.
Quote: “And this paper has major problems. None of those problems, with one exception I’ll clearly mark as such, are nitpicky or particularly complicated or debatable. They all bear on the fundamental validity of this paper … ”
“I’m going to run down the five issues I find most concerning in this preprint, plus a bonus sixth that may or may not be a fair criticism: potential HARKing; unexplained loss to follow-up; a boatload of unaccounted-for confounds; an introduction of more confusion about what puberty blockers are for (confusion that is now bordering on extreme and inexplicable; the potentially unjustified lumping together of kids from clinics that have different protocols and/or outcomes); and the possibility that the researchers used an inappropriate statistical technique.”
I always ask, and in this case it is worthwhile :
WTF IS LGBTQ+
… it is telling, I think, that the relevant surgeries involved never Include inserting a prostate gland – perhaps this is anticipated in a synthetic human future… perhaps removal of the prostate is an option, but even in that case …
WTF IS LGBTQ+
[ answer : The synthetic dialectical identity of a Gnostic cult religion to subvert same-sex marriage laws in the United States ]
“I am not sure how this affects the 25 other states that do not have laws against medical affirmative care; those states have not passed bills banning it (or, presumably, allowing it) that can be adjudicated at the nation’s highest court.”
The decision means states are free to regulate, or not regulate, gender affirming medical care, subject to having a rational basis for any regulation but no regulation is required.
But now with the issue on the table and in our consciousness, I think moderates and conservatives in some blue and especially purple states can petition to have similar legislation voted for or against in election years.
As Jerry’s last paragraph notes, a number of European countries have “severe restrictions on affirmative care.” That seems a more moderate position than an outright ban. My understanding is that one condition in at least some of these countries is close follow-up when procedures are approved after due diligence. This would appear to allow for collection of evidence about at least some of the unknowns about trans care, ideally with good quality studies. A ban precludes this and appears to be based on a predetermined conclusion that the outcome is always or almost always harmful and that harmful outcomes cannot be prevented with “appropriate” restrictions as adopted in parts of Europe. Seems to border on ideological, religious or otherwise.
Interesting overlap with cases where decisions must be made about whether child should be raised as girl or boy due to ambiguous sex organs or damage. The best known case of the latter is perhaps the controversial one of David Reimer (from Manitoba where I live) who lost his penis due to a circumcision accident. He was raised as a girl and was initially reported by John Money as successful and evidence for the socialization of sex identity. But Reimer later assumed a male identity, even married, and ultimately committed suicide after some major setbacks. I’m not familiar with the current status of such conditions.
“Puberty blockers are banned in the UK to treat gender dysphoria in under-18s.”
https://healthmedia.blog.gov.uk/2024/12/11/puberty-blockers-what-you-need-to-know/
IANAD, but I don’t think it’s appropriate to perform surgery on a baby or small child simply because of ambiguous sex organs, and as far as I know it isn’t done anymore. The old-fashioned practice of “assigning a sex”* to such children and then surgically altering their genitals is now seen, rightly, as barbaric.
I think there are some disorders of sexual development that can actually present medical problems. Boys with Swyer Syndrome, for example, (XY gonadal dysgenesis), won’t undergo puberty without hormone replacement therapy.
*That’s where that phrase comes from.
Young people with Swyer Syndrome (46,XY Complete Gonadal Dysgenesis) aren’t properly called boys, because “the ambisexual
gonads fail to differentiate into testes, and remain as
non-functional streak gonads.” (*
Since sex isn’t defined in terms of chromosomes, their “XY-ness” doesn’t make them male. Given that they have neither testes nor ovaries, people with Swyer Syndrome aren’t objectively classifiable as either male or female.
(* Hutson, John M. “Abnormal Embryology in DSD.” In Disorders of Sex Development, ed. by John M. Hutson, Garry L. Warne, & Sonia R. Grover, 41-52. Berlin: Springer, 2012. p. 41)
You’re right; I shouldn’t have referred to children with Swyer Syndrome as boys. Per Wikipedia, they have an inactive SRY gene, or it’s lacking altogether, so they actually develop internal female organs (except for ovaries.) They’re treated with estrogen and progestogen. Thanks, Oliver.
I truly wish for the medical profession to develop standards of care in this area based on the best evidence—and devoid of ideological considerations. I know that this is a lot to ask, but it should at least be their aspiration.
Having legislatures do the job of the medical establishment seems inappropriate to me. The courts—while they tend to decide only if legislated statutes are constitutional or not, rather than on the medical merits—nonetheless impinge on the medical treatments themselves. Neither legislatures nor the courts really have the necessary expertise to connect the right treatments to the right patients.
Maybe the above is too many words. The essence of it is that I wish the medical profession would get its act together so that the government doesn’t need to practice medicine on their behalf.
The medical profession did establish standards of care in this area. See WPATH’s SOC 8. While one may object because they perceive WPATH as an advocacy group, the medical community embraced that SOC. Consequently, I believe the medical community has itself become an advocacy group, and only the public can prevent this through its elected officials.
Yes, you are correct. Medicine is not a law unto itself. The state permits it the privilege to self-regulate in the public interest. But only as long as it holds up its end of the bargain. It is illegal for a doctor to do female genital mutilation and he must report, as child abuse, if he knows someone plans to transport a child out of the country to have it done in a foreign country. Sex-trait manipulation in minors with drugs and surgery falls into the same breach of trust. The state is right to act.
My worry hearing people objecting to the state interfering with trans medicine is that they don’t realize just how toxic and ill-founded this treatment is. The information is ample to ban it as mutilation. (I don’t know how the U.S. federal government works for medicine but there is nothing, except blind ideology of course, to stop Canada’s federal government from banning gender-“affirmation” in the Criminal Code nation-wide the same way it criminalizes FGM and “conversion therapy.”)
Bravo to the defence team who made their case to the Supreme Court and Bravo to the six Justices.
It seems reasonable to classify “gender affirmation” treatment as an extreme type of conversion therapy. That’s even its official purpose in Iran.
Has anyone else noticed that the NYT has begun using the term “puberty-delaying” medications in place of “puberty-blockers?”
Did the Supreme Court actually ignore whether identifying as transgender counts as being a protected class? It seems they upheld the ruling that it doesn’t and some of the justices added explanations why.
For example, on X Christina Buttons cites several passages and summarizes them:
https://x.com/buttonslives/status/1935414851549175880
The ruling also significantly mentioned the loose and contradictory definitions of “transgender.”
I think Pediatric Sex Trait Modification is an extreme treatment for what’s clearly a culture-bound diagnosis for nebulous feelings of discomfort. Just as Intelligent Design was hampered from using emotionally persuasive tactics once forced into courts of law, the same appears to be happening to “not feeling like your mind matches your sex.”
Thanks for this; I went by the National Law Review’s summary, which said that, and did not read the whole decision. And good for Christina.
Also pondering this after reading SCOTUS language. Seems like comps to ascriptive/immutable class defining characteristics need to be dismissed out of hand. If not you invite trans-racial, trans-species, trans-ageism etc classes to affirm rights and treatments and protections on the same basis. Left with an internal perception of mental events the path forward seems to lie in sorting out the involuntary urges of sexual orientation (biological and usually unchanged) from volitional and/or emergent but changeable (ie by puberty or exposure to gay lifestyles). The advocates who pretend otherwise is to the demise of their goal. I don’t have the answer, but the western world knows enough about this phenomenon now and it’s huge social contagion driver to be unconvinced by simple civil rights appeals.
Transgender might survive as a protected class under the narrow employment-discrimination rubric. I believe this is referred to as “Bostick” where the Supreme Court held that an employer couldn’t fire someone merely for “being trans.” If you allow a woman to wear a dress appropriate for business you can’t fire a man for wearing one. But if you require all employees to wear overalls, hard hats, and safety boots, the trans employee can’t claim a gender-expression exemption that the hard hat doesn’t go with her feather boa and she shouldn’t have to take the assigned duty that requires it. The Tennessee law regulates health care, not employment.
Nonetheless, that some Justices referred to trans identity as mutable suggests (to me) that this protected employment category could fail, also. “If you want this job badly enough, you’ll stay out of the ladies’ room because they don’t want you in there. And no, we’re not renovating the plumbing just for you. Save your gender expression for your own time.”
Since I referred incorrectly to “Bostick” — it’s actually Bostock v. Clayton County — I include this piece from today to elaborate.
https://lgbcouragecoalition.substack.com/p/the-supreme-court-just-ruled-states
The other day, NPR has a big news bit about this and of course their slant was as predicted. This and commentary on other issues of the day lay bare just how far over to the left is this national public radio service. These instances nowadays alternate with urgent messages to support NPR against the threat that its federal funding will soon be cut off.
I love my NPR, and really I don’t mind that it is so slanted (as it’s amusing, and their schtick is conversation-worthy), but I have to reluctantly agree that it is wrong for unmatched taxpayer dollars to go to a major mouthpiece of one extreme side of one political party.
I heard the NPR report on the SC decision, and did not find it slanted at all
https://www.npr.org/2025/06/18/nx-s1-5421276/scotus-transgender-kids-decision
Nina Totenberg mentions the dissenting arguments, but those are perfectly interesting and deserve to be considered. I thought it was notable that the dissent had to do with the technicalities of discrimination rather than the biology, psychology, or sociology — that was hardly an “extreme side of one political party.”
Jerry writes, “In the future, I think medical gender-affirmative cafe will, along with our poor treatment of farm animals, be seen as practicers that were immoral in their time, but widely practiced”.
I know “gender-affirmative cafe” is a typo but it’s a sort of on-the-nose metaphor for many gender clinics:
Distressed girls and their worried parents edge up to the clinic counter, and after a bit of banter about waiting briefly for your drink to cool (and after a lot of money goes into the till), the MD barista readies a Lupron latte with two pumps of testosterone and a reminder to come back soon.
That’s very good, Mike. Do you mind if I post the cafe’s business model on a Slack I follow? I’ll leave your name off, or cite you if you prefer.
Go for it!
My understanding is that the dissenting argument was basically “if a boy has an endocrine disorder then he gets testosterone in order to look more like his true identity of ‘boy,’ but if a girl wants to get testosterone to look more like her true identity of ‘boy,’ she’s denied it. This is sex discrimination !”
I don’t agree with the assumed analogy.
Thanks I appreciate your more thoughtful analysis (compared to my frivolous cafe contribution). I think the analogy breaks down because the phrase “endocrine disorder” in the first part of your summary is missing from the second part. A girl who says she has the true identity of a boy doesn’t have an endocrine disorder. There’s a normative idea: a boy’s endocrine system is supposed to generate a lot of testosterone, and if his doesn’t then he has a medical disorder for which a physician would normally be expected to offer treatment; but a girl’s endocrine system is not supposed to generate a lot of testosterone (only a little), and if hers doesn’t then this is not evidence that she has a medical disorder, and a physician should not offer the same treatment that would be offered to a boy.
Is that what you had in mind about the assumed analogy?
[edit to add: Violating those norms is I think what many activists have in mind when they talk or write about queering medicine.]
Yes, that’s well put.
The opposition, however, has accused this reasoning of being an example of the Naturalistic Fallacy – that what’s natural or intended by Nature is best. As they translate the issue, we’re saying a boy’s body is supposed to generate large amounts of testosterone but it’s unnatural and thus wrong to put large amounts of testosterone’s in a girl’s body. We must support Nature and prevent human choices.
This means that anyone making the reasonable distinction between an endocrine disorder and a mental state of feeling disordered (fixing the one with medication and the other with therapy) is being Just Like the Religious — a point of view popular among atheists worshipping at the altar of Autonomy.
With apologies for overcommenting:
Great that’s helpful and I see what you mean. The Naturalistic Fallacy claim makes sense, but only if one ignores the leap from what a physician would normally be expected to offer to treat an endocrine disorder (testosterone in the boy) to what a physician would normally be expected to offer to treat a mental disorder (counselling in the girl). The argument isn’t that high testosterone for boys is normal and therefore good. The argument is that low testosterone for girls is normal and therefore not to be treated medically by a physician. There’s no good-bad value judgement involved. I think that’s the error the genderists are making (and trying to hide)?
Instead of making that error, a libertarian genderist could argue for delisting Lupron and testosterone so that a girl with normal low testosterone could masculinize herself without the involvement of a physician. [edit to add: She doesn’t need a physician to prescribe lifting weights, cutting her hair short, wearing a ball cap backwards, or adopting other masculine stereotypes.] Andrea Long Chu came closest to making that argument in New York Magazine last year.
https://nymag.com/intelligencer/article/trans-rights-biological-sex-gender-judith-butler.html
In my next life I want to enrol in a course you teach, Mike.
Thank you for this elegant analysis Mike. You’ve given me food for thought.
Emily Yoffe’s article is good, as always: summarizing the case (which I’ve mostly read by now) well. I particularly like the lobotomy comparison and use it a lot myself in the many arguments I’ve had in this area. (The trans horror actually cost me most of my family.. a long boring sad story I’ll spare you, though I’d been researching it for some years before, ever since 2017.)
She’s right we’ll look back on all this with horror. Another comparison is the Repressed Memory era of the 80s where thousands of innocent parents had their lives ruined, many jailed, by the crazed ideas of children weaponized by society. From that came the Satanic Panic – which was less serious though better publicized. And over a century ago thousands of women had hysterectomies for similar insane reasons. It was another social mania. I have a collection of others.
The FFRF is more of a yesterday’s force after the splashy and excellent departure of our host and our classic liberal friends like Pinker and Dawkins.
D.A.
NYC
You can hear a short snippet at 29 minutes from a detransitioner as she recounts what it feels like to be on testosterone.
One reason, among many, for why you cannot perform satisfaction surveys on young folks going through these procedures. So much of the “evidence” used to support these interventions are short term self assessments by vulnerable cohorts getting high on drugs and social media affirmations.
While I am delighted with this Supreme Court ruling, I remain a bit dismayed. The advocates have many of us arguing about how best to treat transgender youth. In doing so, they have won the first and most important battle: getting people to accept through frequent use of language that “transgender” is a material reality.
I am still waiting for evidence that there is any such biological condition rather than it being a social reinterpretation of natural variance in the male and female populations. Should a “transgender” state be established, then we can talk reasonably about whether and how it needs to be treated.
Me too Doug, I’m waiting for the same Godot.
Doug, critics of radical transgenderism, of the American Academy of Pediatrics, etc., know not to talk about transgender kids. They talk about gender dysphoria, social contagion and trans-identifying kids or youth.
Watch for an upcoming article “Gender Identity: The Career of a Category” to be published in Theory and Social Inquiry. Sorry, it’s embargoed until the issue is published but I think it addresses the very question you ask.
Very good piece in the Times by Confessore about how the Democratic Party got committed to transgender issues.
I agree: the piece is very good.
Here’s an archived copy:
Nicholas Confessore: How the Transgender Rights Movement Bet on the Supreme Court and Lost. New York Times, June 19, 2025
The inside story of the case that could set the movement back a generation.
https://archive.ph/XTAVp
Andrew Sullivan offers his thoughts about United States v. Skrmetti and what a disservice Chase Strangio and his fellow campaigners and allies have done to the gay and lesbian scene with their agressive activism.
https://andrewsullivan.substack.com/p/strangio-things-ab3?r=4yoler&utm_campaign=post&utm_medium=email&triedRedirect=true